Fertility NEWS LETTER
Ideal fertility : ICSI / IVF & Genetic Center India
Vol V Issue 8, Aug 2009
In this issue :
- Blastocyst transfer: A technique to improve success rate in Test Tube baby
- Fellowship course in Reproductive endocrinology and Infertility
In previous issue :
- IVF triplet pregnancy ends in HELLP syndrome with DIC
- A case of achondrogenesis.
- Ultrasound markers of successful pregnancy
|
Dear Colleges
Hello
In this issue I am putting one topic on blastocyst transfer, written by our embryologist.
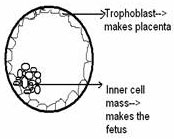
In IVF we fertilize the embryo outside of the body and then transfer them inside the uterus usually on second or third day of fertilization in side the uterine cavity. Normally the fertilized egg enter into the cavity on day 5/6 at the stage of blastocyst( an embryo differentiated into inner cell mass and trophoblast). The covering of the embryo( shell,called zona pellucida ) is stretched out and thin . The trophoblast which makes the placenta proper is just about to come out of the shell at that stage ,hence chances of implantation increases.
But to do a culture or maintain the growth of embryo in laboratory is a very difficult job. The embryo in natural fertilization is not exposed to ambient air. It grows in less oxygen and high carbon dioxide environment. We in our set us ,use culture media in sequential fashion (according to the need of embryonic stages) and create a hypoxic atmosphere around it by using triple gas incubator. The pH of the media is strictly maintained around 7.3 ,this give a good growth of blastocyst.
We are starting on fellowship course in reproductive endocrines and Infertility. It is designed to train those gynecologist who wish to start a proper Infertility clinic. I made it for one week so that they can have a full knowledge of technical and practical aspect of this field.
I wish you all the best
Bye
Dr. D’Pankar Banerji
1. Blastocyst transfer: A technique to improve success rate in Test Tube baby
Dr. Rinku Banerji
Consulting Pathologist and Embryologist
Ideal Fertility : ICSI,IVF and Genetic Center
1st Floor Deshbandhu Complex, Naudra Bridge ,Jabalpur
www.idealfertility.com
In a natural pregnancy, the fertilization occurs in outer part of the fallopian tube. The embryo forms in the fallopian tube and with the peristaltic movements of the tubal musculature, the embryo is pushed towards the uterine cavity and it implants after 5-6 days of fertilization.
In the context of fertilization, be it in-vivo (natural) or In-vitro, the early embryos are dependent of the maternal genome (maternal mitochondria and RNA). The embryos grow well till day2-3 (4- 8 cell stage) and are supported by maternal egg material (yolk). Here all the embryos look same. But further growth only occurs when embryonic genome is activated and only those embryos will make the fetus whose embryonic genome is activated. The embryos may look good on day 2/3 but if its embryonic genome is not activated then it is destined to die. In IVF when more embryos are formed, it is very difficult to distinguish which embryo’s genome will be activated. If day 2/3-embryo transfer is planned then it is very difficult to choose amongst the lot. It might be possible that bad embryos are transferred and good are frozen, as morphologically they look same.
In blastocyst stage transfer, we grow all the embryos till day5 to day6. Here only those embryos will be available for transfer whose embryonic genome is activated and it is independent and sufficient to make a baby if gets implanted. As there is a natural selection and good embryos are available hence the implantation rate will be naturally more. We can transfer less number of embryos and the chances of multiple pregnancies reduce.
Another important aspect of blastocyst transfer is that, the uterus is accepting a day5 embryo in natural pregnancy and it is proved that uterus is best prepared after fifth or sixth day of fertilization for helping in nidation. This shows that blastocyst is the better stage to get a better implantation rate in IVF.
What is the appropriate number of embryos to transfer?
In IVF or test tube baby, when eggs are retrieved in higher number, and the number of embryos formed are more, then it becomes difficult to identify which are good embryos on second or third day of fertilization. And if more number of embryos is transferred then there are higher chances of multiple pregnancies, which is another great danger of IVF.
In our situation we transfer 2-4 embryos depending on the age of the female partner and the embryo grading also. But we try to balance, that the couple should have a pregnancy but should not have multiple pregnancy (> 2 is avoided).
Those couple with a very good chances for pregnancy can be identified on the day of embryo transfer and can be offered the option of transferring two or three embryos. In our situation in these cases we achieved 70-72% pregnancy rate with blastocyst transfer
Blastocyst culture and transfer:
An embryo that has developed for five to seven days after fertilization and has developed 2 distinct cell mass and a central cavity filled with fluid called blastocyst cavity. The surface cells that surround the cavity is called tropho ectoderm and destined to form the placenta and the inner cell mass is destined to form baby proper.
A healthy blastocyst will begin hatching from its outer shell by the sixth or seventh day. Shortly after hatching from the shell, it should begin to implant into o the lining o f the mother’s uterus.
In the past it was difficult o get good numbers o f high quality blastocysts with in-vitro culture systems. However advanced culture media have been developed that provide the proper balance of nutrients at the various stages of early embryo development. In our setting we use sequential culture media and use low oxygen atmosphere to improve the culture conditions and that yields excellent blastocyst formation rate.
But there is some disadvantage also in blastocyst transfer technique. Some time, no embryo crosses the day2/3 embryonic block and we don’t have any embryo to transfer on Day 5 (Here our policy is to go for blastocyst only for those couple when there are more than 4,
good day 3 embryos, otherwise day 3 transfer is followed).
2. Fellowship course in Reproductive endocrinology and Infertility
Course Objectives :
To provide a detailed refresher of endocrinology from basic science to clinical practice. To update the practitioners in Reproductive medicine. To help them to start an Infertility unit so that they can do IUI to IVF,ICSI in future. To interact with them through out the day to solve their queries and to learn from them too.
Target Audience :
Post Graduates and Practicing Gynecologist who wish to start Infertility Unit.
Program :
DAY 1
THEORY :
Basic reproductive endocrinology of female, Understanding of Hypothalamo-pituitary-gonadal axis
PRACTICAL:
Microscopy, stereozoom, trinocular, micro-photography and documentation ,inverted microscope and micromanipulator introduction
DAY 2
THEORY
Introduction to cell biology and cell division and cell culture, Meiosis and Gametogenesis, Culture media preparation
PRACTICAL:
Tissue culture media preparation for IUI
DAY 3
THEORY
Basic endocrinology of Male, Hormonal control of Spermatogenesis
PRACTICAL
Routine semen analysis, sperm preparation methods for IUI, hands on
DAY 4
THEORY
Anovulation and Polycystic ovaries ,Hirsutism
PRACTICAL
Preparation of culture dishes and droplet making under oil
DAY 5
THEORY
Amenorrhoea ,How to deal with it.
PRACTICAL
Hands-on retrieval of mammalian eggs and their in vitro maturation
DAY 6
THEORY
Induction of Ovulation for IUI and IVF
PRACTICAL
Observation and demonstration of Cryo preservation techniques
- Theory classes will be from 9.30am to 11.00am.
- Candidates can repeat their practical, if they wish
- Candidates will be involved in daily OPD infertility counseling and treatment approach from 11-4 . They will see and do transvaginal sonography (as patients allow).
- They will be allowed to observe IVF and ICSI procedures done during their stay. They will have access in embryology laboratory to see the lab set up and equipments and exposure to embryology ( observation), fertilization to blastocyst stage and embryo transfer.*
- Fees : Rs .25,000 per candidate. Students** : Rs.15,000
- One or Two candidates are allowed in one batch
- Course will be from Monday to Saturday of a week.
- Certificate of attendance will be given at the end of the course
- Prior registration is must with full payment( demand draft in the name of Dr.D'Pankar Banerji,payable at Jabalpur)
- Stay and food is extra. Stay @ Rs. 500-1500/day can be arranged in nearby hotels within one kilometer of the venue
Faculty :
Dr.D'Pankar Banerji, Consulting Gynecologist and Infertility specialist
Dr. Mrs. Rinku Banerji ,Consulting Pathologist and Embryologist
Venue : Ideal Fertility, ICSI,IVF and Genetic center, Jabalpur
Depending on the availability of cases.
Student, applies to undergraduate medical students and residents. A letter from the Head of the Department proving the participant’s student status must accompany each student registration.
| Archives |
- Vol VIII, Issue 11, Nov 2010
- Vol VIII, issue 6, June,2010
- Vol VIII,issue 5, May 2010
- Vol VIII,issue 4, April 2010
- Vol VIII Issue 3, March 2010
- Vol VIII, Issue 1,Jan 2010
- Vol VII, Issue 12,Dec.2009
- Vol VII, Issue 11,Nov.2009
- Vol VII, Issue 10,Oct.2009
- Vol VII, Issue 9, Sep.2009
- Vol VII, Issue 8, Aug 2009
- Vol VII, Issue 7,July 2009
- Vol VII, Issue 6,June 2009
- Vol VII Issue 4 april 2009
- Vol VI, Issue 9, Sep 2008
- Vol Vi Issue 8, aug 2008
- Vol Vi Issue 7, july 2008
- Vol VI, Issue 6, June 2008
- Vol V, Issue 17, may 2008
|
- Vol IV, Issue 16, April 2008
- Vol III, Issue 15, March 2008
- Vol I & II, Issue 13-14, Jan Feb 2008
- Vol IV, Issue 12, December 2007
- Vol IV, Issue 11, November 2007
- Vol IV, Issue 10, October 2007
- Vol IV, Issue 9, September 2007
- Vol IV, Issue 8, August 2007
- Vol IV, Issue 7, July 2007
- Vol IV, Issue 6, June 2007
- Vol IV, Issue 5, May 2007
- Vol IV, Issue 4, April 2007
- Vol IV, Issue 3, March 2007
- Vol IV, Issue 2, FEB_2007
- Vol IV, Issue1, Jan 2007
- Vol III, Issue 9, Nov Dec 2006
- Vol II, issue7, July 2005
- Vol II, Issue4 April 2005
- Vol II, Issue3, March 2005
|
|